My MRI Shows a Disc Bulge. Do I Need Surgery?
A disc bulge is one of the most common findings in the human spine, and on its own it is rarely a reason to operate. Here is what your report actually means.
Almost every week, someone sits across from me holding an MRI report, worried. They have read the words disc bulge, and somewhere between the scan centre and home, that phrase has quietly turned into a fear of surgery. The first thing I usually tell them is this: a disc bulge on a report is one of the most common findings in the human spine, and on its own it is rarely a reason to operate.
Let us walk through what a disc bulge actually is, what your MRI is really telling you, and when surgery genuinely needs to be part of the conversation. The goal here is not to dismiss your concern. It is to replace worry with a clearer picture, the same way I would explain it if you were sitting in front of me.
- A disc bulge is a common, usually mild finding, and on its own it rarely means surgery
- Around half of pain-free 40-year-olds have a disc bulge on MRI, so the scan describes the spine, not necessarily the pain
- Most disc-related back and leg pain improves with conservative care over weeks to months
- When a true herniation occurs, the body often shrinks it on its own, and the larger ones resorb the most
- Surgery is for selected, persistent, or severe cases, not for a word on a report
- New bladder or bowel changes, saddle numbness, or worsening leg weakness need same-day care
A disc bulge on an MRI report often causes more anxiety than the finding itself. MRI scans are valuable tools, but they must always be interpreted alongside symptoms, physical examination, and how the problem affects daily life.
What exactly is a disc bulge?
Between each pair of bones in your spine sits a disc. Think of it as a small cushion with a soft centre and a tougher outer ring. These discs absorb load every time you bend, lift a gas cylinder, sit on the floor for a meal, or ride your two-wheeler over a rough road.
A disc bulge means the disc has spread slightly beyond its normal border, a little like a tyre that has softened with years of use. It is broad and gentle, not a dramatic event. This is different from a disc herniation or prolapse, where a more focal piece of the disc pushes out and can press on a nerve. Many people use the words interchangeably, but on a report they are not the same thing.
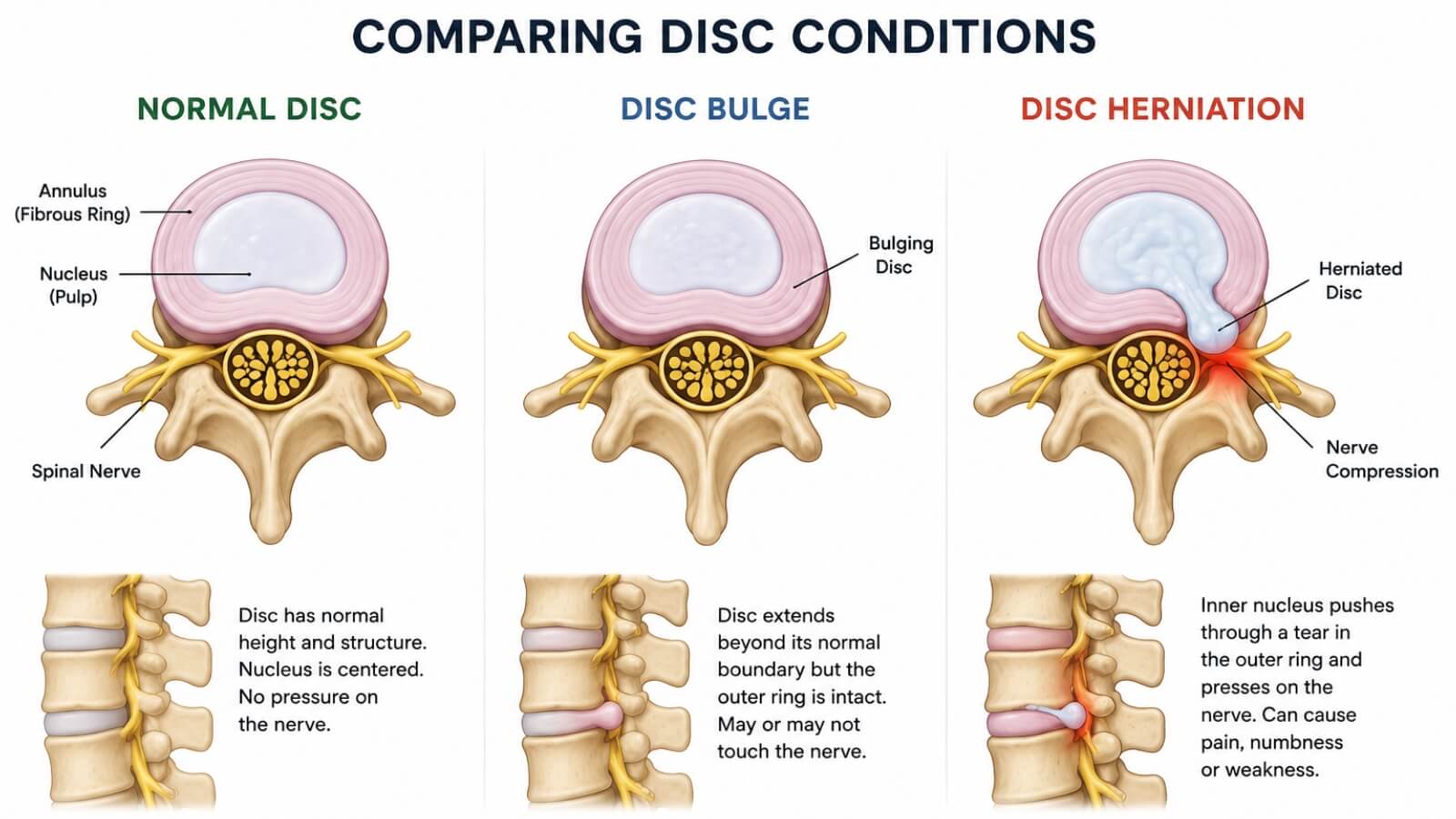
A disc bulge remains contained within the outer ring of the disc, while a disc herniation involves disc material pushing through the outer layer and potentially irritating a nearby nerve. Understanding this difference helps explain why many disc bulges do not require surgery.
A bulge is usually the gentlest finding, often just a sign of a spine that has been working for a few decades. A herniation is more focal and is the type more likely to irritate a nerve. The distinction matters, because most of the fear around the word "bulge" really belongs to the more dramatic herniation, which is itself often treatable without surgery.
What is the truth about MRI reports?
Here is the fact that surprises most patients, and it is worth reading twice. Disc bulges are extremely common in people who have no back pain at all.
A large systematic review published in the American Journal of Neuroradiology in 2015 looked at MRI scans of more than three thousand people who had zero back pain. It found that around half of pain-free 40-year-olds already had a disc bulge, and by 50 that figure rose to about 60 percent. Broader disc wear, called disc degeneration, was present in roughly two out of three pain-free people in their forties.
Read that again. These were people with no pain, no complaint, living normal lives. If you scanned a hundred healthy people walking around a market in Chennai, a large number would have a disc bulge on MRI and never know it. So finding one on your scan does not, by itself, explain your pain or sentence you to an operation.
When a patient shows me a report with "disc bulge" underlined in worry, I usually put the report down first and ask what they actually feel, when it started, and what makes it worse. Then I examine them properly. Only after that does the scan get its turn, as one piece of evidence among several. The report is where the conversation starts, not where it ends.
Why do MRI findings and pain not always match?
An MRI is a photograph of structure. It shows what your spine looks like. It does not show what your spine feels, and it cannot point to exactly which finding, if any, is causing your symptoms.
This is why two people can have almost identical scans and completely different lives. One has constant pain. The other plays with grandchildren and climbs temple stairs without a thought. The scan is the same. The person is not. This is also the heart of our conservative-first approach: a report describes the spine in general, but treatment has to be built around you, your symptoms, your examination, and how the problem behaves in daily life.
Can a disc bulge cause symptoms?
Yes, sometimes it can, and it would be wrong to pretend otherwise. A disc bulge can contribute to back pain or stiffness, and if disc material presses on a nearby nerve it can cause pain, tingling, or numbness travelling down the leg. That leg symptom is what people often call sciatica.
But contributing to a problem and being the whole problem are two different things. Most back pain is mechanical, meaning it comes from how the back is loaded and used: posture, long hours of sitting, repeated bending, and a routine that never gives the spine a break. A familiar local example is the ache that builds up from long two-wheeler rides through Chennai traffic. In these cases the bulge on the report is part of the background, not the villain. The honest position is that a bulge may be relevant, and the job of a careful examination is to work out whether it actually is.

Everyday activities such as long two-wheeler commutes, repeated bending and lifting, and prolonged floor sitting often contribute more to back pain than MRI findings alone. Understanding these daily loading patterns is an important part of managing mechanical back pain.
When does a disc bulge become serious?
A disc problem becomes genuinely serious in a small number of situations. The clearest warning signs are not about the size of the bulge on the report. They are about what your body is doing.
If there is real weakness in a leg or foot that is getting worse, numbness spreading around the groin or saddle area, or any new change in control of the bladder or bowel, that is a different category altogether and needs urgent attention. We will come to these red flags in detail below, because knowing them is what allows you to relax about everything else.
Does every disc bulge need surgery?
No. This is the single most important line in this article. The vast majority of disc bulges never need surgery.
There is also a fact about the spine that very few patients are ever told, and it is genuinely reassuring. When there is a true herniation, the body often clears it away on its own. Research that tracked herniated discs over time found that the more dramatic herniations frequently shrink without any operation. In one well-known review, the largest, most alarming-looking extrusions resorbed in around 70 percent of cases, and the very biggest, most displaced fragments in even more.
In plain terms, the scan that looks the scariest is often the one most likely to settle by itself. That is the opposite of what most people assume when they read their report. Surgery removes the disc material with an operation. In a large number of people, the body was going to handle a good part of it anyway, given time and the right care.
What treatments are usually tried first?
For a disc bulge, and even for many true herniations causing leg pain, the first line of treatment is almost always conservative, meaning without surgery. This is not a delay tactic. It is what the evidence supports, and it is what works for most people.
Conservative care usually includes a few simple things working together:
- Staying gently active. Complete bed rest is one of the oldest myths in back pain. Lying flat for days makes the back stiffer and weaker. Gentle movement and short walks are usually better medicine.
- Adjusting daily load. Looking honestly at what aggravates it, such as long two-wheeler rides, repeated heavy lifting with a bent back, or hours of sitting without a break, and modifying those for a while.
- Physiotherapy and targeted exercise. A structured physiotherapy programme to build core and back support, introduced step by step, helps both recovery and prevention.
- Short-term pain relief. Simple medicines and measures such as a warm hot water bag can take the edge off while the body settles.
Most episodes of disc-related back and leg pain improve substantially over a few weeks to a few months with this kind of patient, consistent approach.
I often see patients who have stopped almost all activity out of fear of their scan. They have read the report and decided the spine is fragile. That fear usually does more harm than the bulge itself, because the back gets weaker and stiffer with disuse. The goal is sensible, guided movement, not avoidance.
When should surgery actually be considered?
Surgery has a real and valuable place. The point is not to avoid it at all costs. The point is to use it for the right person at the right time, not as an automatic response to a word on a report.
The largest study comparing surgery with non-surgical care for disc herniation, known as the SPORT trial, is useful here. It studied people who already had genuine nerve-related leg pain that had persisted for at least six weeks. It found that both groups improved. Those who had surgery improved faster and a little more, and that benefit held for years. But many people who did not have surgery also recovered well.
So for ordinary, non-emergency cases, surgery is mainly a question of how quickly you want relief, weighed against the fact that the problem often improves on its own with time. It is a reasonable choice for someone whose leg pain is severe, disabling, and simply not settling after a fair trial of conservative care. It is not something to rush into because a scan sounds frightening.
If surgery has been advised for a disc bulge without a proper trial of structured conservative care, or if you feel rushed and uncertain, a second opinion is reasonable. A bulge alone, without persistent disabling symptoms or red flags, rarely demands an operation, and it is fair to understand all your options first.
What are the red flag symptoms that should not be ignored?
There is one situation where waiting is the wrong choice, and every patient with back trouble should know it. Knowing these signs is not meant to frighten you. It is the opposite. Once you can recognise the genuine emergency, you can stop worrying about the things that are not.
- New difficulty passing urine, or loss of control of the bladder or bowel
- Numbness around the groin, genitals, or the saddle area that would touch a seat
- Weakness in a leg or foot that is clearly getting worse, for example a foot that begins to drag
- Pain, numbness, or weakness travelling down both legs at once
These can be signs of significant nerve compression that needs prompt assessment. They are uncommon, but they are the exception that genuinely cannot wait. If you ever notice them, do not sit at home wondering. Get examined immediately.
What I tell patients in clinic
When someone shows me a report with the words disc bulge underlined in worry, I slow the conversation down. I ask what they actually feel, when it started, what makes it worse, and how it affects their day. Then I examine them properly. Only after that does the scan get its turn, as one piece of evidence among several.
A scan can describe your spine. It cannot describe you. The report is where the conversation starts, not where it ends.
Most of the time, that conversation ends with relief rather than a surgery date. We agree on a sensible plan, give the body time and support to do what it does well, and keep a clear eye out for the few warning signs that would change the plan. That is conservative-first orthopaedics. Surgery stays available as a tool for the people who truly need it, and not as a default for everyone who owns a frightening report.
Frequently asked questions
Is a disc bulge the same as a slipped disc?
Not exactly. A bulge is a broad, mild spreading of the disc and is usually the gentlest finding. A slipped or herniated disc is more focal and is more likely to press on a nerve. People use the terms loosely, but on a report they describe different things.
Does a disc bulge mean my spine is damaged?
Usually not in the way people fear. A bulge is very often a normal sign of a spine that has been used for years, much like grey hair or a few wrinkles. Around half of pain-free 40-year-olds have one and never know it.
Can a disc bulge heal on its own?
Symptoms from disc problems very often settle on their own with time and sensible care. When there is a true herniation, the body frequently shrinks the disc material naturally over months, and the larger ones tend to resorb the most.
Will my disc bulge get worse if I do not have surgery?
For most people, no. Avoiding surgery does not mean the problem marches on unchecked. The majority improve with conservative care, and a bulge is not a ticking clock as long as none of the red flag symptoms are present.
Is it safe to walk or exercise with a disc bulge?
In most cases, yes, and gentle activity usually helps. Staying still for long periods tends to make the back stiffer. The right kind of movement, often guided by a physiotherapist, supports recovery rather than threatens it.
Can I lift heavy things or sit on the floor with a disc bulge?
You can usually return to normal life, but technique matters while things settle. Lifting with a straight back and bent knees, and breaking up long periods of floor sitting or bending, reduces strain. The aim is sensible loading, not permanent restriction.
Do I need to repeat my MRI?
Often not. Repeating a scan rarely changes the plan unless your symptoms change significantly or a red flag appears. How you feel and how you move matter more than a new photograph of the same disc.
Will I end up in a wheelchair if I avoid surgery?
This is a common fear and it is almost always unfounded. A simple disc bulge does not lead to paralysis. The only situation that carries that kind of risk is the red flag picture described above, which is rare and needs urgent care, not routine worry.
How long does recovery take without surgery?
It varies, but most disc-related back and leg pain improves significantly over a few weeks to a few months with consistent conservative care. Recovery is often gradual rather than sudden, and patience is part of the treatment.
Is bed rest good for a disc bulge?
No. Prolonged bed rest is one of the most outdated ideas in back care. A day or two of relative rest during a severe flare is reasonable, but beyond that, gentle movement helps far more than lying down.
Should I get a second opinion before agreeing to spine surgery?
If surgery has been advised and you feel rushed, confused, or uncertain, a second opinion is a completely reasonable step. A bulge alone, without persistent disabling symptoms or red flags, rarely demands an operation, and it is fair to understand all your options first.
Can a disc bulge disappear on MRI?
In some cases, yes. Disc herniations and protrusions can partially shrink over time through a natural process called resorption. Improvement in symptoms is often more important than changes seen on repeat MRI scans.
Practical take-home points
- A disc bulge is common and is often a normal sign of ageing, not damage.
- Around half of pain-free 40-year-olds have a disc bulge on MRI.
- The scan describes your spine, but treatment must be based on you and your examination.
- Most disc problems improve with conservative care, and many herniations shrink on their own.
- Surgery is for selected, persistent, or severe cases, not for a word on a report.
- Learn the red flags. New bladder or bowel changes, saddle numbness, or worsening leg weakness need same-day care.
- If you have been advised surgery and feel unsure, a second opinion is reasonable and wise.
Worried about a disc bulge on your report?
If your MRI mentions a disc bulge and you are not sure what it means for you, it is worth having it explained in the context of your actual symptoms. Conservative-first, with digital X-ray and in-house physiotherapy on site.
WhatsApp Dr. Sumesh to EnquirePatients from Thirumullaivoyal, Ambattur, Avadi, Annanur, Pattabiram, and nearby areas commonly seek consultation after being told they have a disc bulge on MRI. In many cases, careful examination and conservative treatment remain the most appropriate first step.
When to consult Dr. Sumesh Subramanian at OrthoCure, Thirumullaivoyal
If you are holding an MRI report that mentions a disc bulge and you are not sure what it means, it is worth having it explained properly, in the context of your actual symptoms rather than the words on the page. This is especially true if your pain is not settling, or if surgery has been suggested and you would like a calm, conservative-first opinion before deciding anything.
Dr. Sumesh Subramanian consults at OrthoCure Bone and Joint Speciality Clinic, Thirumullaivoyal, serving Ambattur, Avadi, and Annanur, with dedicated spine and neck pain care, digital X-ray, and in-house physiotherapy on site, so assessment and a clear plan can usually happen in a single visit.
If any of the red flag symptoms described above are present, please do not wait for an appointment. Seek medical care immediately.
This article was medically reviewed by Dr. Sumesh Subramanian (MS Orthopaedics) and last updated on 17 June 2026.
Medical References
- Brinjikji W et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. American Journal of Neuroradiology, 2015. — Source for disc bulge prevalence in pain-free people by age (around 50% at age 40, 60% at age 50).
- Chiu CC et al. The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clinical Rehabilitation, 2015. — Source for spontaneous resorption rates of disc herniation by type.
- Weinstein JN et al. Surgical versus Nonoperative Treatment for Lumbar Disc Herniation: the Spine Patient Outcomes Research Trial (SPORT). JAMA, 2006; with 4-year and 8-year results in Spine, 2008 and 2014. — Surgery versus conservative outcomes in persistent radiculopathy.
- NICE Clinical Knowledge Summaries and AANS guidance on cauda equina syndrome. — Source for red flag symptoms requiring urgent assessment.