Knee Pain While Climbing Stairs or Getting Up From a Chair: What It Means, and What Helps
Most common explanation: Patellofemoral pain (kneecap joint overload). This is very common in office workers, homemakers, and anyone who alternates long sitting with sudden stairs.
Quick self check: Pain is mainly at the front or around the kneecap, worse on stairs or chair rise, and often better on flat walking.
At OrthoCure Bone and Joint Speciality Clinic, Thirumullaivoyal, I see this pattern daily in patients from Ambattur, Avadi, Annanur, Iyyapakkam, and nearby areas. Many people try rest and pain tablets, feel better briefly, then the pain returns the moment stairs, squatting, or floor level sitting comes back. The long term fix is usually not a stronger tablet. It is a better plan: smarter load management, stronger hip and thigh muscles, and better movement control.
What the evidence says (in plain words)
- Stairs and chair rise dramatically increase kneecap joint load compared with flat walking, which is why symptoms show up there first.
- Hip and quadriceps strengthening is first line and consistently improves pain and function in most adults with patellofemoral pain.
- Imaging is not routinely required unless there are red flags, a major injury, or failure to improve with a structured plan.
Get checked early if you notice any of these red flags
- Swelling that keeps returning, or a visibly puffy knee.
- True locking (the knee gets stuck and will not straighten).
- Repeated giving way, or sudden falls because the knee “lets go.”
- Fever, severe night pain, redness, or a “hot” joint (rare, but urgent).
- Pain after a significant fall, twist, or sports injury.
- What this pain pattern usually means
- Why stairs and chair rise feel worse
- “Chondromalacia” vs patellofemoral pain: what MRI words really mean
- Patellofemoral pain vs early knee osteoarthritis: how they differ
- How we diagnose it, and when imaging helps
- Proven non surgical treatment plan
- Taping, bracing, and foot support: when they help
- Medicines (including NSAIDs): the short term role
- How long does it take to improve?
- When to see an orthopaedic doctor
- Frequently asked questions
- References
What this pain pattern usually means
Your kneecap (patella) sits in a groove at the end of the thigh bone (femur). Whenever your knee bends under load, pressure rises behind the kneecap. Stairs, squats, and standing up from a chair are classic examples.
If the kneecap joint becomes sensitive, or if the hip and thigh muscles are not controlling the movement efficiently, load shifts onto the front of the knee and pain becomes noticeable. This is commonly called patellofemoral pain or anterior knee pain.
Important point: this does not automatically mean arthritis, and it does not automatically mean surgery. Many patients have normal X rays and still have significant stair pain. In these cases, the problem is usually a load and control issue, not a structural emergency.

Why stairs and chair rise movements hurt more
Stairs and chair rise load the knee when it is bent. A bent knee increases pressure at the kneecap joint, and the movement demands strong hip and thigh muscles to share the load. If muscles fatigue, or control is inefficient, the kneecap joint works harder and pain appears in a predictable way.
Common real life triggers in Chennai routines
- Apartment stairs, footbridges, or metro station steps.
- Standing up from a low sofa, low chair, or floor sitting.
- Indian toilets or deep knee bend positions.
- Repeated chair rise during household work and caregiving.
- Long office sitting, then sudden stairs (classic flare).

“Chondromalacia” vs patellofemoral pain: what those MRI words mean
Many patients get anxious because an MRI report says “chondromalacia patella”. In simple terms, this often means the cartilage behind the kneecap looks irritated or softened.
Key clarity
- Patellofemoral pain is a clinical diagnosis: symptoms plus exam findings.
- Chondromalacia is an imaging description: what the MRI sees.
- You can have chondromalacia words on MRI and still recover very well with conservative care.
- This is not the same as “advanced arthritis” in most adults.
Patellofemoral pain vs early knee osteoarthritis: how they differ
Both conditions can cause pain with stairs, but the overall pattern is often different. This matters, because the management focus is different.
Typical differences (not absolute rules)
- Patellofemoral pain: pain mainly at the front of the knee, worse with stairs and chair rise, often better on flat walking.
- Early osteoarthritis: may include stiffness (especially morning or after rest), swelling episodes, pain in multiple areas of the knee, and sometimes pain even on flat walking.
- X rays can be normal in patellofemoral pain, and can also be early/near normal in early OA. The exam and story are still critical.
If you are over 40 and symptoms include stiffness, swelling, or broad knee pain (not just the front), an X ray may help clarify whether early osteoarthritis patterns are present.
How we diagnose it, and when imaging helps
In most adults, diagnosis is clinical. The pain pattern and a movement assessment usually explain the cause. Imaging is used to rule out other problems when it truly changes the plan.
What we assess in clinic
- Front knee tenderness and kneecap tracking.
- Hip strength, quadriceps strength, and control on a step down or sit to stand.
- Signs suggesting early arthritis patterns, tendon irritation, or meniscus issues.
- Biomechanics: does the knee collapse inward under load?
When X ray or MRI is useful
- X ray: age over 40 with stiffness or swelling, broad knee pain, or suspicion of osteoarthritis.
- MRI: true locking, recurrent giving way, significant swelling, major injury, or no improvement after 6 to 12 weeks of a proper rehab plan.
If you need quick imaging support, see: Digital X ray in Thirumullaivoyal.
Proven non surgical treatment plan
High quality evidence supports conservative management as the first line for patellofemoral pain. The pillars are: education, load management, and hip plus quadriceps strengthening.
Step 1. Calm the flare, but keep moving
- Reduce repeated stairs temporarily if pain is high, but do not stop all activity.
- Avoid deep squats and very low chair rise for now.
- Use supportive footwear on hard floors, especially at home.
- Use short term pain relief only as support, not as the main treatment.
Step 2. Strengthen the hip and quadriceps (the core solution)
The knee is where you feel it. The hip and thigh are often where the solution starts. Better hip abductors and external rotators reduce inward collapse, and better quadriceps control improves shock absorption at the kneecap joint.
What helps most adults
- Quadriceps strengthening with correct form (pain guided).
- Hip abductor and hip extensor strengthening.
- Step control training (especially step downs) to improve alignment.
- Gradual load progression, not sudden “back to normal” jumps.
Step 3. Return to stairs with progression (not bravery)
The goal is not to avoid stairs forever. The goal is to improve your capacity so stairs do not trigger a flare. A graded return is usually the fastest safe route back to normal life.
For supervised rehab and technique correction, see: Physiotherapy in Thirumullaivoyal.
Taping, bracing, and foot support: when they help
These supports can reduce pain in the short term for some people, especially during stairs or long standing days. They work best as “helpers” while you build strength and control.
- Taping: can provide short term pain relief in some patients, often by improving patellar tracking cues.
- Knee sleeve or patella support: may improve comfort and confidence; it does not replace strengthening.
- Footwear and insoles: helpful if you stand long hours on hard floors or have foot mechanics that increase knee load.
Medicines (including NSAIDs): the short term role
Medicines can reduce pain and help you participate in rehabilitation. However, they do not correct the load problem by themselves. If a medicine helps you do exercises and move better, it is doing its job.
Common approach
- Short term NSAIDs may be used if there is a painful flare, provided you have no contraindications.
- Use gastro protection when needed, and avoid long term self medication.
- If pain is recurrent, the priority is structured rehabilitation, not repeated tablets.
How long does it take to improve?
Many adults notice meaningful improvement within 6 to 12 weeks when they follow a consistent strengthening and load management plan. If symptoms have been present for months, improvement can still happen, but it may take longer.
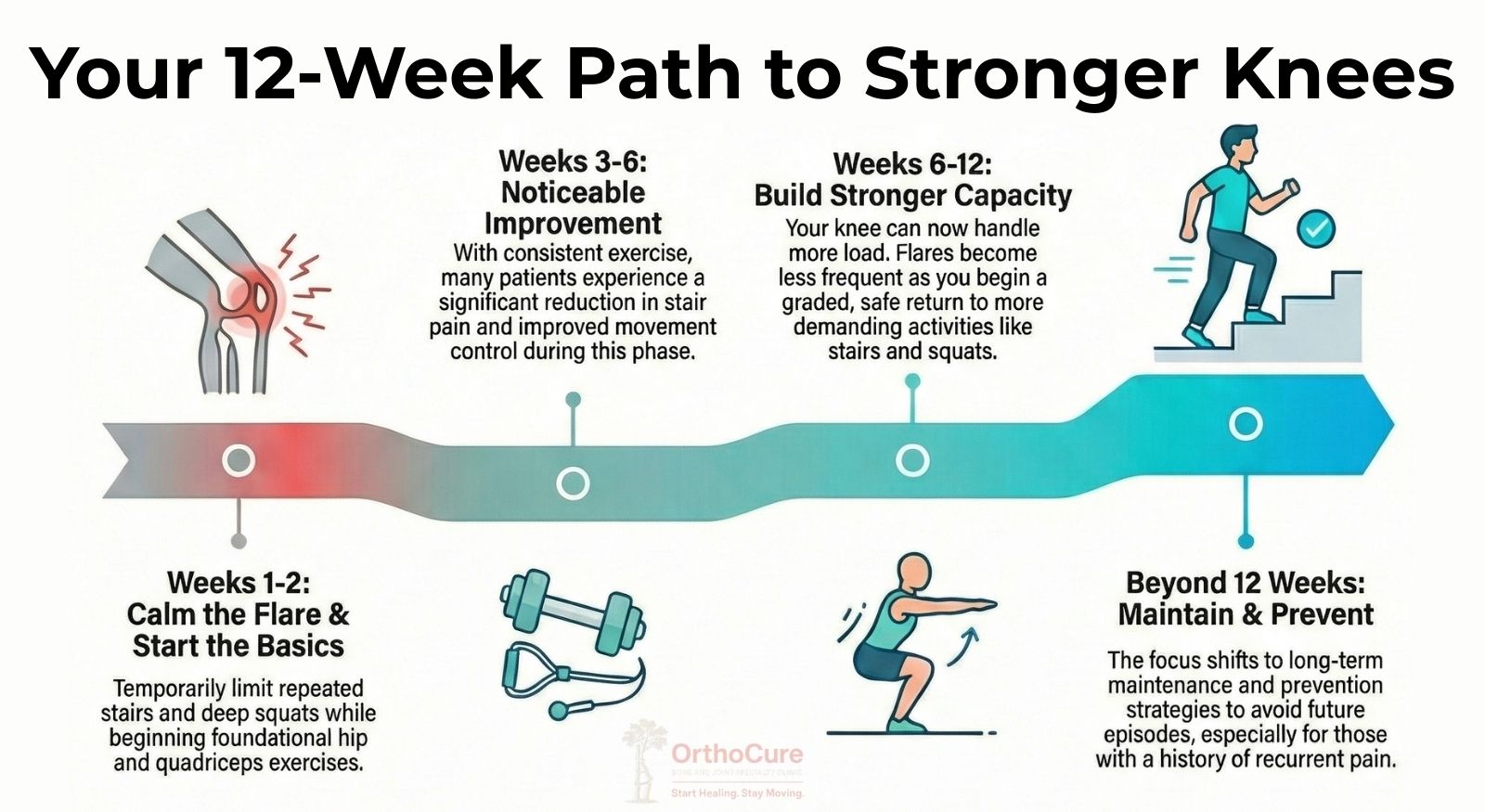
A practical timeline you can expect
- Weeks 1 to 2: pain control, trigger reduction, start basic hip and quadriceps work.
- Weeks 3 to 6: noticeable reduction in stair pain for many patients, improved control.
- Weeks 6 to 12: stronger capacity, fewer flares, graded return to stairs and squats.
- Beyond 12 weeks: maintenance and prevention, especially for those with recurrent episodes.
When to see an orthopaedic doctor?
Consider a clinical review if any of the below is true:
- Pain persists beyond 2 to 3 weeks despite sensible activity changes.
- Stair pain is worsening week by week.
- Swelling, locking, or giving way is present.
- Night pain, fever, redness, or severe rest pain is present.
- You want a clear plan instead of trial and error.
A focused clinical examination usually clarifies whether this is patellofemoral overload, early osteoarthritis patterns, tendon irritation, or another cause. The earlier you correct the load problem, the faster you break the recurrence cycle.
Want a clear plan for knee pain on stairs in Thirumullaivoyal?
If stairs or getting up from a chair is triggering knee pain, the fastest path forward is a focused assessment and a practical plan. Most cases improve with targeted strengthening, load management, and better movement control.
At OrthoCure Bone and Joint Speciality Clinic, Thirumullaivoyal, we focus on conservative recovery first, with imaging only when it truly changes the plan.
Clinic hours: Monday to Saturday 5:00 PM to 9:00 PM. Sunday 11:00 AM to 1:00 PM.
No. 2, 2nd Street, Santhipuram, Thirumullaivoyal, Chennai 600062.
Serving Thirumullaivoyal, Ambattur, Avadi, Annanur, Iyyapakkam, and nearby areas.
Frequently asked questions
Is this arthritis?
Not always. Knee pain that is clearly worse on stairs and chair rise is commonly a patellofemoral overload pattern. Arthritis becomes more likely with age, stiffness, swelling, or pain across multiple parts of the knee. A clinical examination is the quickest way to separate these patterns.
Should I stop walking?
Usually, no. We reduce flare triggers temporarily and build strength so walking becomes easier, not frightening. Controlled activity is typically better than complete rest.
Will a knee support help?
It can help some patients in the short term, especially during stairs or long standing days. It works best as a temporary support while you improve strength and movement control.
Do I need an MRI?
Not in most cases. MRI is considered when there is true locking, recurrent giving way, significant swelling, a major injury, or failure to improve after a structured rehab plan.
References (for medical accuracy)
The page is written in patient friendly language, but the principles below reflect mainstream, evidence based guidance and research on patellofemoral pain and rehabilitation.
- Best practice guide for patellofemoral pain based on synthesis of a systematic review, the patient voice and expert clinical reasoning. British Journal of Sports Medicine, 2024. (Best practice synthesis). View
- 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis. British Journal of Sports Medicine, 2016. (Consensus). View
- Is patellofemoral pain a precursor to osteoarthritis? British Journal of Sports Medicine, 2018. (Review). View
- Effects of aging on patellofemoral joint stress during stair ambulation. Journal of Biomechanics, 2024. (Biomechanics). View
- Hip strengthening prior to functional exercises reduces pain sooner in patellofemoral pain. Journal of Orthopaedic and Sports Physical Therapy, 2011. (RCT; foundational). View
- Quadriceps or hip exercises for patellofemoral pain? Randomised controlled equivalence trial. British Journal of Sports Medicine, 2023. (RCT). View
Medical disclaimer
This article is for education only and does not replace a clinical examination. If you have severe swelling, fever, inability to bear weight, true locking, or worsening night pain, please seek urgent medical evaluation.